Big spike in respiratory illness, psychedelics for depression, addiction treatment, and screening for lung cancer
December 9, 2022

Happy Friday,
Today, I’ll discuss the current surge of respiratory illness, new efforts to get employers to sponsor psychedelic drug treatment for depression, the continuing shortage of accessible addiction treatment, and a report that the wrong people are often being screened for lung cancer.
1. Influenza and COVID-19 rates up, and RSV still causing havoc at children’s hospitals
It’s been a bad month or more for respiratory viruses in the US. Influenza hospitalizations now exceed COVID-19 hospitalizations, and while RSV (respiratory syncytial virus) hospitalization rates are coming down, they remain much higher than in any previous year. Pediatric hospitals are still jammed with babies needing respiratory support for RSV. Most RSV deaths are in the elderly, and it will take some time before we know the mortality impact on this population.
The following charts show the enormous difference in 2022 compared to previous years:
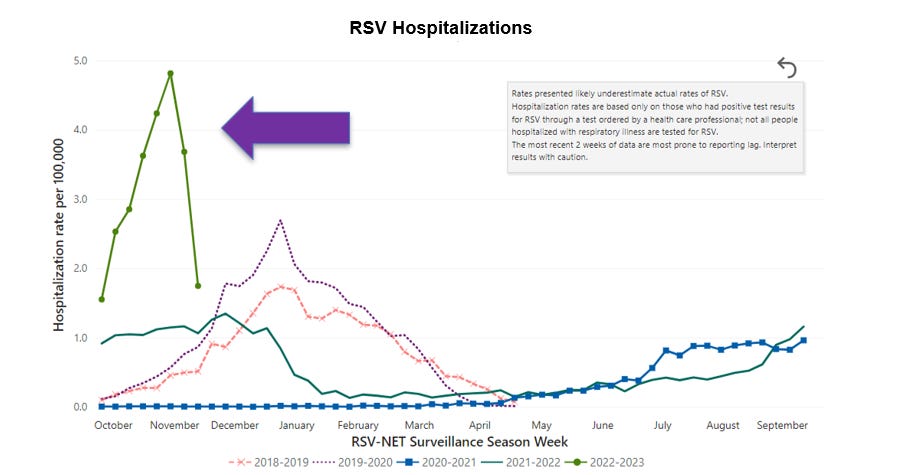
Source: Centers for Disease Control and Prevention (CDC) December 7, 2022 LINK
Note that the last data point, showing a steep drop, could be incomplete.
Influenza Hospitalizations

Source: CDC 12/7/22 LINK
The red line shows how much earlier we are seeing influenza hospitalizations, which typically start to rise at the very end of the year. It’s unclear if the influenza ‘season’ will end early, like it did in the Southern Hemisphere, or if it will just start early and end in the usual timeframe, i.e. February – March.
COVID-19 Hospitalizations

Source: CDC 12/7/22 LINK
We are nowhere near our 2021 Omicron peak, but hospitalizations are up 29% in the last two weeks. Wastewater surveillance from the last 2 weeks shows large increases, which suggests that the number of infections and future hospitalizations will increase in the final weeks of 2022.
Some have misleadingly focused on reports that those who are vaccinated (and even boosted) represent a larger portion of COVID-19 deaths than they did last year. The vaccinated (and boosted) continue to represent a smaller portion of deaths than expected, and vaccination rates are higher among seniors, who are at the highest risk of dying. Here’s an explainer on this from KFF (Kaiser Family Foundation). This week there was also good news on vaccinations preventing childhood and adolescent hospitalizations and deaths, improved laboratory and real world protection from bivalent boosters, and a thoughtful opinion piece suggesting extra COVID-19 vaccination during pregnancy to protect infants.
Implications for employers:
- Employers can expect Q4 medical costs to be high due to the exceptional amount of medical care being delivered to address the current “tripledemic.” Unlike during peaks of the COVID-19 pandemic, hospitals are not generally canceling adult elective surgery, although some facilities are having difficulty maintaining staffing levels.
- Employers should continue to encourage both influenza vaccination and the bivalent COVID-19 vaccine. The evidence continues to gather that boosting prevents COVID-19 hospitalizations and saves lives. Vaccines help us maintain capacity in our hospitals and emergency departments. Here's a link to a new toolkit for employers to encourage bivalent COVID-19 vaccines from the Health Action Alliance.
- Use of Paxlovid continues to be very low, and those who are over 65, unvaccinated, immunocompromised or have other risk factors should be treated promptly upon diagnosis. Paxlovid is now distributed at no cost by the federal government, although this will become the responsibility of employer-sponsored health insurance next year barring new Congressional funding.
- The CDC Director has recommended resuming masking in crowded places, although the CDC has not implemented new mask requirements. While few employers will return to mask requirements at this point, all should make employees feel comfortable wearing masks in the workplace.
- Employers can lower workplace risk of infection by maintaining excellent ventilation, which helps prevent spread of influenza, RSV, and COVID-19.
- Workers with paid time off or sick leave are less likely to come to the workplace when they are most likely to transmit respiratory viruses
2. Psychedelics can help with treatment resistant depression, but the FDA approved drug is expensive and can be hard to find.
There is a growing body of evidence that psychedelics are effective for some people who have depression that have not been successfully treated by other means. Ketamine, an intravenous antidepressant, has been used off-label for this for many years. A component of ketamine, esketamine (Spravato) nasal spray was approved for treatment-resistant depression in 2019, although this has not been used widely because it requires observed administration 1-2 times a week for eight weeks. A course of therapy costs over $7000. This therapy is approved for those who have major depression and are acutely suicidal, and is generally reserved for those who would otherwise be treated with electroconvulsive therapy, which is effective but sometimes has serious side effects.
National carriers generally provide coverage for Spravato with prior authorization, although some private clinics don’t accept insurance and charge patients $8-10,000 out-of-pocket for a course of therapy. A new third party administrator, Enthea, recently got $2 million in seed funding and has announced intentions to provide a set of credentialed providers for this service to employers, positioning this as a perk for progressive employers.
Clinical trials are underway to determine effectiveness of psilocybin (psychedelic mushrooms) for depression, and MDMA (otherwise known as Ecstasy) for post-traumatic stress disorder.
Implications for employers:
- Employees may already be accessing psychedelics out of pocket through in-person treatment centers or through vendors who sell directly to patients.
- Some employees will be able to gain access to esketamine through conventional health plans. Others might be treated with intravenous ketamine which is far less expensive, but not FDA approved for this indication.
- I view this therapy as an important clinical tool, although I don’t think it should be considered a “workplace perk.”
3. Opioid deaths continue to devastate America
There were over 100,000 reported deaths from opioid overdoses in the US in 2021, fueled by continued contamination of heroin, cocaine and other drugs with high-potency fentanyl. A longform article this week in the Washington Post, “Drugs killed 8 friends, one by one, in a tragedy seen across the U.S.,” and an accompanying podcast tells the story of the deaths of 16 young people in Greenville, NC, who died of drug overdoses in the last decade. This problem knows no geographic, class or racial bounds; my children are both well over a decade out of high school, and both of them have lost high school classmates to drug overdoses, too.
As we have yet to adopt a national plan for the epidemic of drug overdoses, Congress will be considering an investment in improving substance use treatment, although this is not likely to pass in the current lame duck session. Many other developed countries have reduced their toll through harm reduction including better access to mental health treatment and medication assisted therapy.
In the meantime, there are important steps that employers can take.
- Be sure that coverage for inpatient and outpatient substance use disorder treatment is available, and require that carriers or third-party administrators demonstrate network adequacy
- Make Employee Assistance Programs readily available, including on-site where practical. Drug addiction wreaks havoc on the lives of family members of those who are addicted, who need support.
- Train managers and supervisors to recognize the stress that substance use disorder can cause in those who are addicted and their families, and to refer to appropriate resources.
3. Few are getting screened for lung cancer, and many of them shouldn’t be screened!
The US Preventive Services Task Force has recommended low dose CT scan screening for smokers and former smokers in 2013, and revised these recommendations slightly in 2021. Researchers analyzed data from over 96,000 people in 20 states who completed the Behavioral Risk Factor Surveillance System (BRFSS)and they found that 86% of those who reported having a screening CT for lung cancer did not meet the criteria for screening. The current criteria are age 50-80, smoked 20 pack years, and were either current smokers or quit in the previous 15 years. Further, only 16% of those who met the criteria actually got the screening test. The researchers used the older guidelines, which were in place when the survey was performed. This study was based on survey responses, not medical records, and some respondents might have reported their risks or their cancer screening inaccurately.

Source: Liu, et al JAMA Network Open, November 21, 2022 LINK
Evidence-based cancer screening tests can save lives but doing cancer screening tests on people who don’t meet the criteria is costly and could lead to medical harm, as false positives can lead to a cascade of unnecessary medical interventions. Low dose CT scans involve radiation exposure and can cause new cases of cancer.
Carriers have difficulty doing prior authorization for this screening test because there is not a claims code for how many lifetime cigarettes a patient has smoked. Providers are not ordering the recommended screening in six out of seven people who would benefit from screening.
Implications for employers:
- Carriers can educate members about the evidence-based recommendations for the most important preventive services, including cancer screening, that is recommended.
- Carriers need to be accountable for wasteful spending on unnecessary lung cancer screenings that are done. Employers should ask health plans how they are curbing unneeded lung cancer screenings, including post-claim audits.
- The National Committee on Quality Assurance HEDIS has announced that it is developing a quality metric for appropriate and inappropriate lung cancer screening tests, expected to be available in 2024.
Hope all have a safe, healthy and happy weekend!