

GLP-1 drugs , like most medical care, do not lower medical costs
May 12, 2025

Summary: GLP-1 drugs do not lead to lower medical costs in the short run and are not likely to lead to lower medical costs even over a longer time horizon unless prices are substantially reduced.
Impact of Coverage of GLP-1 Drugs for Obesity on Medicare Expenditures
Source: JAMA Health Forum Hwang, April 25, 2025
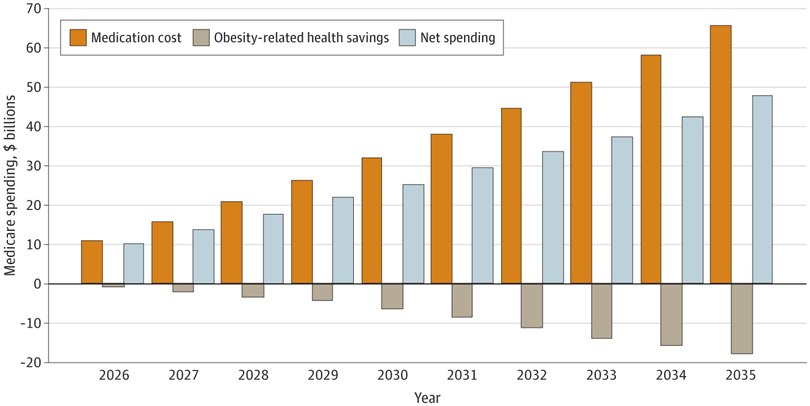
Researchers in JAMA Health Forum used a microsimulation model to assess the likely financial results of Medicare covering GLP-1 drugs for obesity. They found that if the Centers for Medicare and Medicaid Services provided coverage for these medications for obesity, the cost of Medicare Part D plans would rise by $66 billion over the next 10 years, and Medicare plans would get $18 billion in savings from improved health. Therefore, the net impact of the drugs would be an increase in Medicare spending of about $48 billion. Although these drugs would make Medicare beneficiaries healthy, preventing heart attacks, strokes, and kidney failure, the net impact would be higher medical costs. Future models might show more savings as evidence accumulates of additional medical benefits from these medications.
There were some misleading news articles last week that likely misinterpreted some reported data to say that GLP-1 drugs for obesity would be cost saving. The firm has not published data beyond the press release, but it appears that those who take GLP-1s have much higher costs in the first year, and their inflation rate in year two is lower than those not on GLP-1s. I think we’ll eventually see that the total cost of care of those with obesity on GLP-1 drugs is substantially higher than the total cost of care of those who are obese who are not treated with these drugs.
This would be consistent with other research on the impact of GLP-1 drugs for obesity on medical budgets:
Institute for Clinical Effectiveness Research (ICER) 2022: Lifetime cost of drugs $274K; lifetime decreased medical expense $62K
JAMA Health Forum (2025): Showed that the cost per quality adjusted life year (QALY) for tirzepatide (Zepbound) was $197K and the cost per QALY for semaglutide (Wegovy) was $468K. (This study used net costs, not list price, for the drugs). Generally, drugs should not cost more than $100,000 per QALY to be considered cost-effective.
The 2022 New England Journal of Medicine study showing effectiveness of Wegovy at preventing Major Adverse Cardiovascular Events (MACE) required 100 people to be treated for 3 years to prevent one MACE event. The cost of three years of treatment for 100 people at $8,000 a year would be about $240K, and few MACE events would be that expensive.
Most medical interventions that are clinically effective do not lead to future cost savings, exceptions being childhood vaccinations and birth control.
Implications for employers:
Employers should expect coverage of GLP-1 drugs for obesity to improve population health and employee productivity, but the “return on investment” from coverage is not likely to lead to lower medical costs now or in the future.
Lower net acquisition costs for GLP-1 medications would strengthen the economic case for maintaining or adding GLP-1 coverage for obesity. An announcement by one pharmacy benefit manager that it was narrowing its formulary to a single GLP-1 for obesity could help drive lower costs.
Thanks for reading. You can find previous posts in the Employer Coverage archive
Please subscribe, “like” share this newsletter with friends and colleagues. Thanks!
Tomorrow: GLP-1 drugs highly effective in treating liver disease