

Infant mortality, surgical fees, and employer considerations as the pandemic emergency ends
February 17, 2023

Today, I’ll review a study showing stark racial differences in infant mortality - which mirror maternal mortality differences that I’ve discussed in past notes. I’ll present data from a study showing that hospitals that are part of networks have higher fees. I’ll also share a reference to an article that my colleague Patricia Toro, MD MPH and I wrote on employer considerations for the end of the pandemic emergency, and briefly review some other COVID-19 news.
1. Infant mortality is higher in high-income Blacks than in low-income Whites
Researchers reviewed all births in California from 2007 to 2016 to evaluate the impact of income and race on outcomes including birth weight and mortality. They painstakingly correlated each case with administrative datasets to assess race, ethnicity, and income.
Pregnancies in the highest income Black mothers have worse outcomes (higher infant mortality, more prematurity and more low birth weight babies) than the pregnancies in the lowest income White mothers. This is especially distressing because California has done more to improve maternal quality and safety than most states.
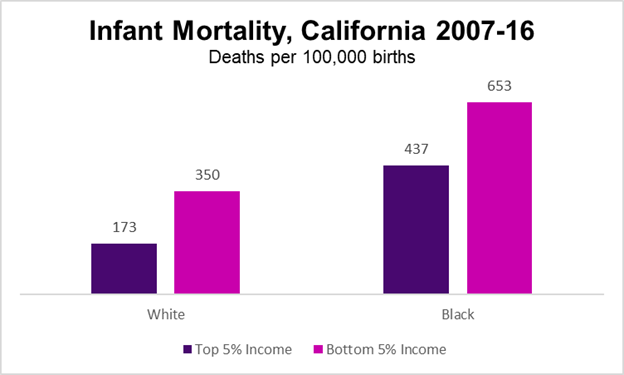
Sources: Kennedy-Moulton, K et al NBER 11/22 LINK and Miller, et al New York Times, 2/11/23 LINK
These researchers also showed that women in the top 5% of income had more preterm deliveries and lower birth weight babies due largely to older age and more multiple births, and that Sweden has consistently larger babies and lower infant mortality and preterm delivery across all income levels.
Health plans, like BCBS-MA have rolled out equity metrics that may start to improve health process and outcome measures based on race and ethnicity.
Implications for employers:
- This is clear evidence that poor Black maternal outcomes are not due to income disparities alone - but are likely due to a combination of social factors, as well as potential racism within the health care system.
- This research also demonstrates that bad maternal and infant outcomes in the US are not limited to low-income women, who are more likely to be covered by Medicaid.
- Employers should continue to press health plans for reporting on quality metrics that includes race and ethnicity to identify these challenges
- Access to doulas can help women of color attain care that is better centered on their perceived needs. Right now, few health plans offer referrals to doulas, and most employers do not subsidize this care.
- Employers can maintain their efforts to get carriers to publish quality and outcome data - which can help all members choose the providers with the best outcomes and encourage better care at providers with worse outcomes. These could also serve as a basis for performance guarantees.
2. Allowable surgical fees are higher at hospitals in networks
When hospitals merge or acquire other hospitals, we often hear about the economy-of-scale advantages and some executives even suggest that consolidation will lead to cost savings.
If only!
JAMA Network Open reports that allowable charges for most selected surgical services at hospitals that are part of a network are statistically significantly higher than at independent hospitals. This is no surprise, and it’s possible that the higher prices are in part because academic medical centers are less likely to be independent.
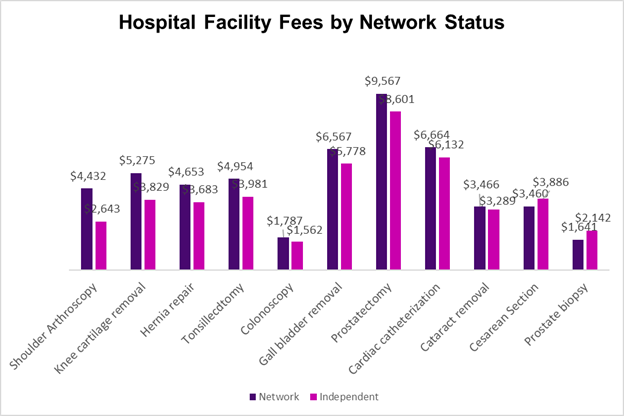
Source: Mullens, et al JAMA Network Open 2/14/23 LINK Costs were higher for all procedures except Cesarean Section and prostate biopsy for hospitals that are part of networks
Implications for employers:
- The federal government’s increased focus on antitrust enforcement could help constrain some price rises, although most health care markets are very considerably concentrated already, and the number of hospitals that are independent is dwindling.
- This is early evidence that new federal transparency rules can provide data to allow policymakers and researchers to better understand health care costs.
3
. COVID-19 news and employer considerations
a) The COVID-19 pandemic emergency will end in May
Employers are considering what actions to take as the pandemic emergency ends. Patricia Toro, MD MPH and I wrote an article covering this in HR Executive that you can share with clients. Here is a KFF summary, and a link to a Q&A I did with the Health Action Alliance. I’ll be participating in a webinar on this subject hosted by Health Action Alliance on February 28 at 2pm ET.
b) New experimental drug is effective in treating COVID-19
Pegylated Interferon Lambda was shown in a large study in Canada and Brazil to dramatically decrease hospitalizations and death from COVID-19. This is especially important since no monoclonal antibodies are effective against the currently dominant variants. The drug is a single injection (doesn’t require an intravenous infusion) and has no more side effects than placebo. It can be used up to 7 days after the beginning of symptoms and is effective regardless of vaccination status. Food and Drug Administration current rules require that clinical tests be performed in the US, so it might be some time before this drug gains emergency authorization in the US.
c) Study shows that Paxlovid is associated with no more rebound than non-treatment
Researchers in Hong Kong evaluated the likelihood of COVID-19 rebound in almost 4500 who were hospitalized, not treated with oxygen, and either got Paxlovid (nirmatrelvir and ritonavir, 242), molnupiravir (563) or neither (3787). They found that there was no significant increase in rebound for those who took Paxlovid compared to those who took molnupiravir or were not treated with an antiviral. While this observational study was among those who were hospitalized, none were treated with oxygen, and thus many of these patients would likely not have been hospitalized in the US.
Those over 50 or immunocompromised should seriously consider Paxlovid in the first five days of a COVID-19 illness
d) COVID-19 associated with increased diabetes diagnoses
Researchers from Cedars Sinai and Brigham and Women’s Hospital found that among adults they treated who recovered from COVID-19 (average age 47), the adjusted likelihood of being diagnosed with diabetes was 60% higher in those who had recovered from COVID-19 in the previous 90 days. The study was large (23,709 patients), and the researchers found no increases in unrelated diseases, so this is likely not simply due to more medical vigilance after recovery from COVID-19. This could be an indicator that we’ll see more cardiometabolic disease in the future in those who have recovered from COVID-19.
e) COVID-19 hospitalization rates continue to be flat in the US
Wastewater surveillance has not changed over the past few weeks, and we continue to see about 450 deaths per day. Deaths continue to be concentrated in those over 75.
Hope all have a great weekend when it comes.
Jeff