Medicare’s alternative payment models increased costs
October 13, 2023

Source: Congressional Budget Office, September, 2023 LINK.
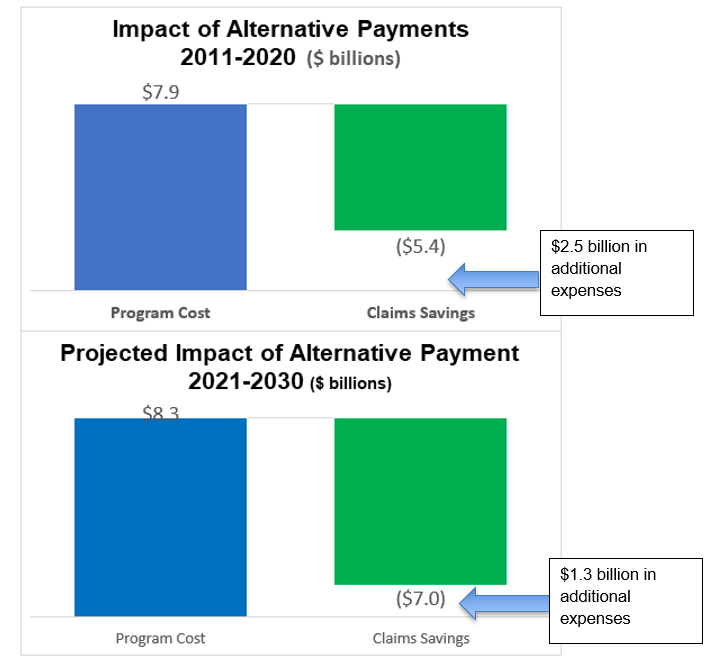
This shows that the alternative payment models increased Medicare costs by $2.5b from 2011-20,
and are projected to increase Medicare costs by $1.3 billion from 2021-2030
Health policy experts generally believe that fee for service reimbursement of providers leads to higher utilization, and many support a transition to alternative payment models, including capitation, bundled payments, and pay for performance. The Affordable Care Act established the Center for Medicare and Medicaid Innovations (CMMI), which is charged with implementing and rigorously evaluating alternative payment approaches. CMMI has implemented 40 payment reform pilots since its inception. If Medicare’s alternative payment model pilot programs lead to lower cost (or higher quality without higher cost), the Center for Medicare and Medicaid Services (CMS) is instructed to expand these pilots. Four of the pilots so far have been shown to save money and expanded.
The Congressional Budget Office (CBO) predicted in 2010 that CMMI would save $1.3 billion in its first decade, and $34 billion in its second decade. A new CBO report tells a different story. Most of the CMMI pilot programs have saved Medicare money in terms of medical claims alone, but these savings have (mostly) evaporated when the cost of ‘bonus’ payments to providers and the cost of administering these programs is considered.
For example, here are the results from CMMI episode payment APMs, reported byMedPAC, the Medicare Payment Advisory Commission.
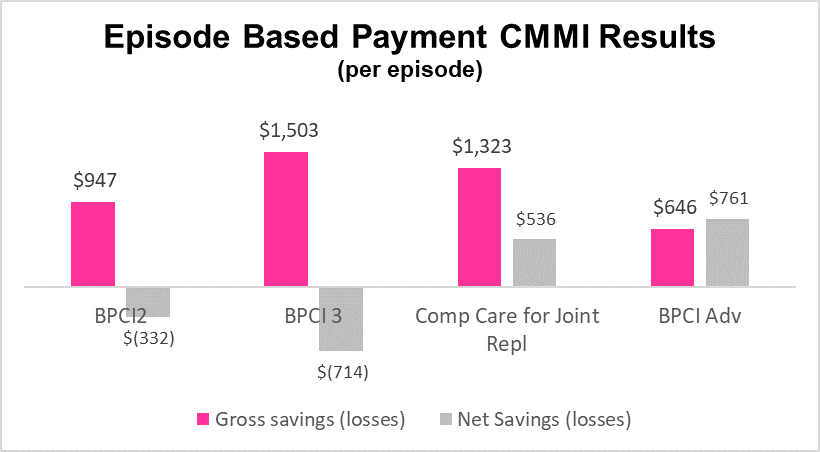
Source: MedPAC June, 2021 LINK BPCI = Bundled Payment for Care Improvement
Implications for employers:
Medicare, which pays for about 21% of total medical costs in the US, is often in a good position to assess new approaches to provider payment. Important CMS innovations such as diagnosis related groups and fee schedules have been widely adopted by commercial health plans.
Rigorous evaluation of changes in payment arrangements must include any bonus or shared savings payments made to providers. Evaluations should also include administrative costs.
Rigorous evaluations of interventions that change provider payment methodology are difficult, require years of data collection and analysis, and are best performed by an independent party. Those who have spent years designing and implementing a program are not in a good position to assess its efficacy.
CMMI has not saved the taxpayers billions of dollars, but the lessons from its first decade can help us as we consider how to improve employer sponsored health plans.
Thanks for reading. You can find previous posts in the Employer Coverage archive
Please “like” and suggest this newsletter to friends and colleagues. Thanks!
Monday: Employer actions can plan a role in decreasing premature heart disease and death