PBMs and carriers often require prior authorization for drugs when specialty society guidelines do not recommend it
September 16, 2025

Summary: Many health plans impose prior authorization requirements for drugs which clinical Society evidence-based guidelines do not recommend utilization management.
Source: Rucker, et al Health Affairs, July, 2025
It’s hard to find anyone that loves prior authorization.
Prior authorization requirements are hated by physicians, who must justify their medical decisions, and by patients, whose care may be disrupted. However, prescribers sometimes don’t prescribe the most cost-effective medications. Low value prescribing can increase out-of-pocket costs and can increase health care premiums for employers and for all health plan members.
Research published in Health Affairs this summer demonstrates that many health plans have imposed pharmaceutical prior authorization requirements that are not consistent with evidence-based medicine. The researchers correlated specialty drug coverage utilization management (UM) requirements of eighteen large commercial health plans with clinical practice guidelines from professional societies compiled by an academic group at Tufts Medical Center. The plans cover about 70% of the commercially insured U.S. population.
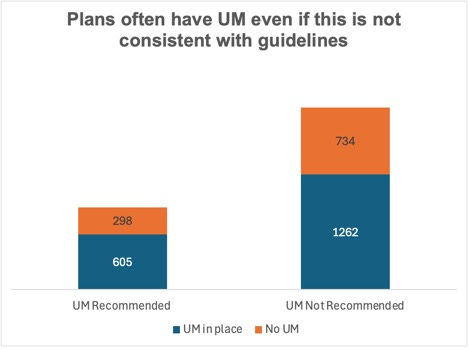
They found that the professional society guidelines recommended utilization management (UM) for only about one-third (32%) of the drug-indication pairs. However, health plans imposed restrictions on clinical use in almost two-thirds of the instances where guidelines did not recommend UM. Restrictions were most often step therapy protocols where a less-expensive drug must be tried first (45%), followed by restrictions on use for certain subgroups (27%).
The researchers focused only on medical carriers and did not review UM requirements imposed by pharmacy benefit managers.
This study shows that there is only a relatively weak correlation between professional society guidelines and health plan UM requirements. Professional societies might recommend UM too infrequently as they represent specialty physicians who feel burdened by the UM process.
In June 2025, most major U.S. health insurers pledged to streamline prior authorization processes as part of a voluntary agreement with the U.S. Department of Health and Human Services. The initiative aims to reduce the volume of services requiring prior authorization by 2026 and implement standardized electronic submission systems by 2027. There are few details about how individual plans will adjust their current utilization management programs, and significant changes are not anticipated until 2026 or later.
Implications for employers:
Carriers often impose UM requirements even if specialty society recommendations do not support requiring prior authorization or other UM
Employers can ask their carriers what they are doing to be sure that their UM programs are consistent with available evidence, and that they are eliminating prior authorization requirements that lead to few changes in therapy.