

Physicians who received drug company payments delivered more low-value care
November 6, 2023

Source: Mitchell, et al BMJ October 25, 2023 LINK
Pharmaceutical companies have been required to report which physicians have received payments (including education, travel and meals) for the last decade. Some of the worst abuses where physician prescribing practice was likely influenced by large payments are safely in the past. Still, last year there were $12.6 billion in payments from pharmaceutical companies to physicians.
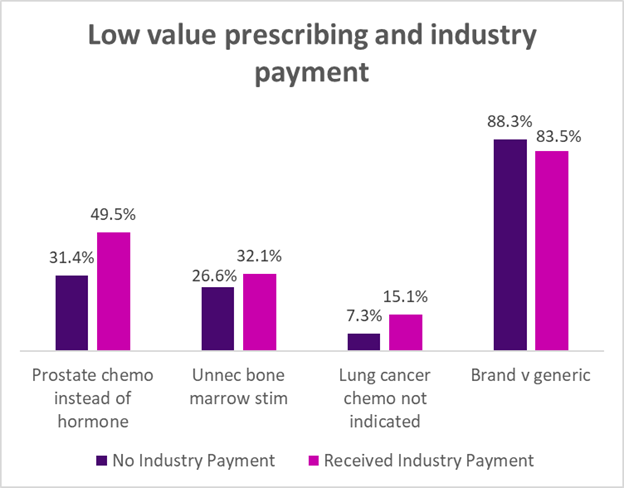
Researchers in BMJ identified four instances where prescriptions for cancer were either low value (such as prescribing a brand name when an equally-effective generic was available) or where the drug was not indicated at all (such as drugs to stimulate the bone marrow when the treatment was unlikely to cause bone marrow suppression). In almost 9000 patients, they reviewed public records of the prescribing physician’s pharmaceutical payments and records of drugs prescribed by that clinician for Medicare patients. They found that about a third of oncologists (30%) received some drug company payment, and in three of the four use cases, those oncologists who received drug company payments were more likely to prescribe low value care. The exception was that those who did not receive drug company payments were slightly more likely to prescribe branded medications, which is a surprise. Some of this might be due to biosimilars which technically are not considered “generics.”
Relatively small payments to physicians can influence their prescribing choices. The median payment in this sample was between $60 and $156.
This research demonstrates an association between low value prescribing and industry payments, but does not establish causality.
Implications for employers:
- For many conditions, there are a range of prescription drugs that would be appropriate. In many instances, less expensive drugs, including generics and biosimilars, are as good as more expensive treatment. But even where there is good evidence, many clinicians prescribe low value drugs, which increase the cost of care without adding value to patients, and sometimes endanger patients.
- Providers hate utilization review, but prior authorization for non-emergency care can prevent some inappropriate prescribing. As I noted last week, poorly-implemented prior authorization creates enormous heartache for those being treated for cancer.
- I was happy to see that 70% of clinicians received no pharmaceutical company payment, and transparency has decreased the number of physicians who accept industry payment.
- Employers should ask their carriers what they are doing to decrease low value care.
Tomorrow: The economic burden of untreated mental illness
Thanks for reading. You can find previous posts in the Employer Coverage archive
Please “like” and suggest this newsletter to friends and colleagues. Thanks!