Preventing overdose deaths, site-of-service payment differentials, higher quality hospitals can save lives, and protection from COVID-19 vaccination and masks
February 24, 2023

Happy Friday!
Today, I’ll cover recommendations about preventing narcotic overdoses in the workplace, the excess cost of paying higher rates for routine care delivered in the outpatient hospital setting, a simulation study that shows that lives could be saved if more people had colon cancer surgery at higher quality hospitals. I’ll also provide data from a new study that shows that those who are vaccinated are less likely to get heart attacks associated with COVID-19 infections and discuss masks to prevent respiratory disease.
1. Preventing opioid overdose deaths in the workplace
There were over 100,000 deaths from narcotic overdoses in the US in 2022, and communities across the country are reeling from the impact of fentanyl contaminating illegal drugs like heroin, or being substituted for more expensive narcotics in pills sold illegally. The Food and Drug Administration just recommended that naloxone (Narcan) be made available with no prescription, which could make it easier for family members and those nearby to give drug users this antidote should they lose consciousness and stop breathing. Naloxone is available both as an injection and as a nasal spray; the spray requires no special training, although is more expensive than the injection.
Few employees actively use drugs when they are at work, but workplace overdoses happen, and ready access to naloxone can save lives. The US Surgeon General recommended that employers stock naloxone in first aid kits in 2018, and the National Institute of Occupational Safety and Heath has a guide for employers seeking to provide naloxone for emergency on-site use. Naloxone is already available without a prescription in many states, and this week the Food and Drug Administration voted unanimously to make naloxone nasal spray over the counter, and final approval is expected soon. This change would make the product more accessible; it could be available in vending machines, convenience stores and supermarkets. Future naloxone products could be higher potency and longer duration.
Employees should call 911 whenever naloxone is used, as the narcotic reversal can be short-acting and drug-induced respiratory depression or unconsciousness can return. Some who have overdosed require a second dose before emergency medicine technicians arrive.
Implications for employers:
● Naloxone as part of a workplace first aid kit can save lives. Kits should include at least two doses, and these should be replaced as they expire.
● Employers that provide access to naloxone should develop clear policies and procedures around its use and should communicate clearly to workers.
2. Paying higher rates for outpatient care delivered at hospitals could cost employers and employees an excess $45 billion per year.
Health insurance has long paid more for the same service performed in a hospital outpatient department than the same service performed in an outpatient clinic or a physician’s office. This is not consistent with “paying for value.” This overpayment also encourages further consolidation and loss of competition, as hospitals acquire physician practices to obtain higher rates.
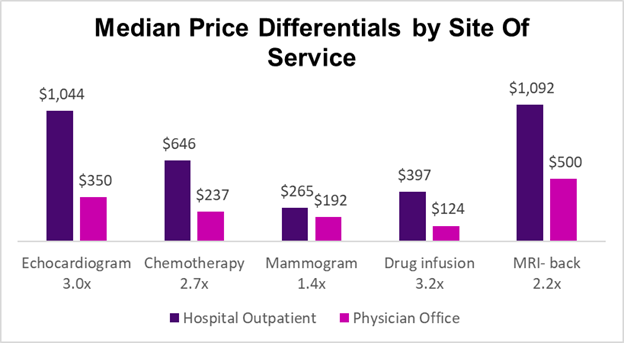
Source: Committee for a Responsible Budget, February 14, 2023 LINK
The Committee for a Responsible Budget reviewed claims data from small, medium and large employers and found that policies to encourage site-neutral payments in the commercial insurance market could reduce national health expenditures by $458 billion from 2024-2033. This could reduce premiums by $386 billion and patient cost sharing by $73 billion.
Implications for employers:
● Employers can encourage carriers to move to site-neutral payment and support proposed state or federal regulations that would require site-neutral payment.
● Employers can consider drug infusion site of care steerage programs offered by their PBM vendor or health plan"
● In the meantime, educating members about out-of-pocket cost savings can help direct some to seek care at less expensive sites.
3. Getting colon cancer surgery at higher quality hospitals could save lives for a very small price.
We know that there are large differences in quality and outcomes among hospitals, and the hospitals with the best outcomes often don’t have the highest prices. Researchers in JAMA Network Open used quality and cost data from Florida hospitals to ascertain what would happen if patients getting surgery for colorectal cancer moved from their chosen hospital to the hospital within 30 miles of their home with the best outcomes. They used 2016-2018 outcome data to “train” their model, and simulated outcomes for those who had colorectal cancer surgery in 2019.
They found that mortality rates at the best-performing hospitals were about a quarter less than those at the chosen hospital on average. Life expectancy was slightly (and statistically significantly) longer. The hospitals with better outcomes were about 2% more expensive, but the extra cost led to more social benefit due to lower death rates. Patients would have traveled 2 miles further from their homes in this simulation.

Source: Finn, et al JAMA Network Open, February 15, 2023 LINK
Implications for employers:
● Health plan members can be directed to higher quality hospitals for a modest increase in cost and little increase in distance from their homes. However, the results from this Florida database are not likely to be applicable to members in rural areas where there are fewer competing facilities.
● Employers still need more accessible data on quality and outcomes to better direct members to the providers with the best outcomes.
● The highest performing hospitals won’t have the capacity for treating all health plan members, so we need to continue to push for quality improvement at all hospitals.
4. COVID-19 Roundup
a) Those who get COVID-19 after vaccination have fewer heart attacks than the unvaccinated.
We know that SARS CoV2, the virus which causes COVID-19, leads to inflammation of blood vessels, and can be associated with heart attack and stroke. Researchers at Mount Sinai Medical School reviewed a US database of almost 2 million who had COVID-19 from March, 2020 to February, 2022, and found that those who were partially vaccinated (a single mRNA vaccine) or fully vaccinated (1 Johnson & Johnson vaccine or 2 mRNA vaccines) had a significantly lower risk of heart attack or stroke in the 180 days after infection. This confirms a Korean study published in JAMA in July.
Implications for employers:
● COVID-19 vaccinations continue to be safe and are especially valuable in preventing heart attacks and strokes in those at highest risk.
b) Masks work to protect individuals, but they have little or no impact on protecting the population at large
There has been a lot of press about a recent Cochrane Review of randomized controlled trials (RCTs) of public masking to prevent spread of influenza and COVID-19. Cochrane reviews are exceptionally rigorous, and this review covered just twelve randomized controlled trials - a tiny fraction of all the studies of masks, but the only ones that were RCTs. The reviewers concluded that over the population there was not compelling evidence that masks decreased the spread of respiratory disease. They noted that the total numbers were small, so they were not certain of this conclusion.
Katelyn Jetelina in her newsletter Your Local Epidemiologist has done a thorough review of this article and surrounding literature. She points to one epidemiologist who re-ran the COVID-19 only studies (4 of the 12) without the influenza studies and found that all showed about a 20% decrease in infection, and two were statistically significant.
My conclusion is that the literature and experience still support mask use to provide individual protection, and demonstrates that well-fitting masks of electrostatic material (like N95 and KN95) provide more protection than loose fitting masks (like cloth and surgical). However, masks likely don’t significantly reduce the spread of COVID (or influenza) through the entire community, in part because people don’t wear masks as directed even if there is a mandate in place.
Implications for employers:
● There is still value of making the workplace “mask friendly,” especially since there is no longer an available monoclonal antibody to protect those with weak immune systems.
● I’m still going to wear a well-fitting and comfortable mask when I’m in crowded indoor spaces when there is widespread community transmission. But I recognize the level of protection might well be lower than I once thought, and I think many with a higher risk tolerance than I have will rationally decide not to wear a mask.
● This evidence does not support future mask mandates to protect the community.
Hope all have a great weekend. If you liked this note, please like, subscribe and recommend to others!
Jeff