Providers are billing for few asynchronous E-visits
January 24, 2024

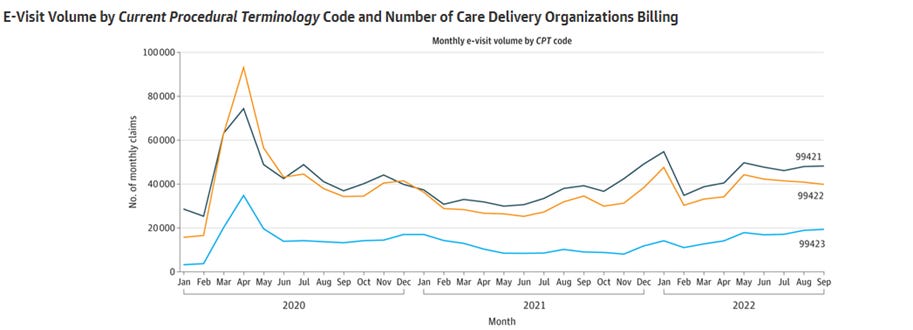
Source: Holmgren, et al JAMA Network Open, January 10, 2024 LINK
Online patient portals are enormously useful. As a patient, I can check results of laboratory tests, make an appointment, download my immunization history, and even ask a question of my physician. However, many patients using a portal to substitute for an office visit increases provider burnout, and doctors complain of “pajama time” answering patient queries after hours. Further, loss of revenue from replaced visits could destabilize some primary care practices.
Some provider organizations, including the Cleveland Clinic, announced that they will begin charging patients for some physician responses, especially those that are time-consuming for the physician. Charging patients could decrease the number of complex questions that burden providers, help providers feel more valued, and improve practice finances. This could also increase the number of unnecessary office visits and frustrate patients, especially those on high deductible health plans.
Researchers in JAMA Network Open reviewed a large claims database (Trilliant Health, with over 270 million unique individuals in each year) and found that billing for these asynchronous visits was infrequent (0.1% of all office visits), and has not increased very much. They also found that most bills were for the lowest intensity of service, taking 5-10 minutes. The most common diagnoses for these low intensity E-visits were sinusitis, urinary tract infection, and respiratory infections. The most common diagnoses for the most intensive E-visits, lasting over 20 minutes, were high blood pressure, viral exposure, and no abnormal findings.
This research was only for asynchronous visits. Many providers are also now billing phone call encounters as low-level visits, which may have been bundled into the reimbursement for in-person office visits in the past.
Implications for employers:
E-visit billing can cause member friction, when members don’t realize that their portal message would lead to a medical bill.
It appears that relatively few of these encounters are leading to charges, at least so far.
Alternative payment models can incorporate a management fee that would incorporate these E-visits.
Employers can ask their health plans to routinely report on billing for asynchronous visits, along with routine in-person visits and routine virtual visits.
We should continue to monitor billing rates for these codes.
Thanks for reading. You can find previous posts in the Employer Coverage archive
Please “like” and suggest this newsletter to friends and colleagues. Thanks!
Tomorrow: Be cautious in interpreting an Oxford study critical of employer mental health programs