

Shorts: CMS drug price negotiations, trauma fees, shingles and COVID vaccines, MDMA and tirzepatide
August 22, 2024


A) CMS releases negotiated prices for 10 drugs
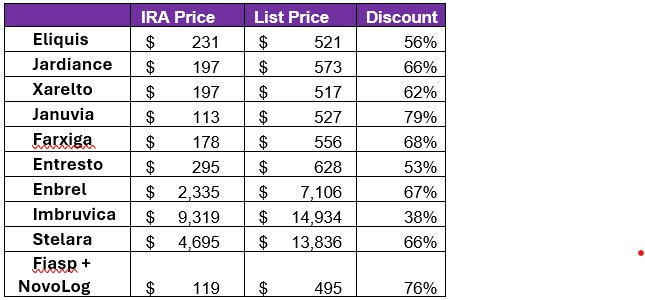
The Centers for Medicare and Medicaid Services (CMS) released the negotiated prices for 10 medications last Thursday morning. Justification for these prices will be released in March, and they will go into effect on January 1, 2026. CMS estimates that this will lower drug costs by $6 billion in the first year. Below is a list of drugs. Note that the actual prices paid currently (after discounts and rebates) is not publicly available; StatNews estimates that most of the drugs will go down in price by about 20%, while three will go down by about 30%. Here’s a link to a past post on implications of the Medicare price negotiations on prices paid by employer sponsored health insurance plans.
I’ll have a full post on the implications of these negotiations tomorrow.
B) Trauma activation fees vary widely
Trauma activation fees are added to emergency department bills for the care of patients who are sick enough that the multidisciplinary trauma team is activated. Emergency departments that are trauma centers must have trauma specialists available at all times, and these fees help them cover the costs.
Researchers report in this month’s Health Affairs that trauma activation fees collected by hospitals vary widely by hospital and by type of payer. Level 1 trauma centers, which take care of the most serious cases of trauma, on average charged commercial payers $5,700, but some charged as much as over $28,000. Private payers were charged twice as much as public payers, but those without insurance faced the highest charges.
Trauma fees were designed to allow hospitals to recoup the costs of keeping trauma teams ready at all times. Hospitals have widened the range of patients that they charge trauma activation fees, and carriers should scrutinize these bills to be sure they are reasonable.
B) Shingles vaccine lowers risk of dementia
Shingles is a reactivation of the virus that causes chickenpox. It is painful and can cause long-term nerve pain. Now, it appears that shingles can predispose to earlier onset dementia, too. Researchers compared the diagnosis of dementia in about 100,000 who had been vaccinated with the older shingles vaccine (Zostrix), and about 100,000 who received the newer, more effective 2-dose vaccine (Shingrix). Those who got the newer vaccine had, on average, 164 days (about five months) longer without a dementia diagnosis. They also had a lower incidence of shingles.
The Shingrix vaccination is recommended for adults ages 50 and older, or 19 and older if immunocompromised.
C) COVID-19 boosters associated with lower risk of heart attacks and blood clots
Researchers reviewed medical records of 45.7 million residents of England[TP(1] , and published their findings in Nature Communication in late July. They found that the likelihood of having arterial or venous blood clots diminished significantly after people had their second or a later booster vaccination. COVID-19 causes substantial vascular inflammation, so those who are less likely to get COVID-19 are less likely to have blood vessel complications. This is one more reason to get vaccinated this fall!
D) FDA rejects MDMA for depression and PTSD
The FDA rejected approval of MDMA for treatment of drug-resistant depression and post-traumatic stress disorder, following the advice of its advisory committee. A medical journal also retracted three studies from researchers from the manufacturer due to concerns about research ethics. This shows the importance of rigorous research, although I’m confident that other psychedelics, and maybe MDMA as well, will be approved in the future as we need more effective treatments for these diseases. Spravato (esketamine) is a psychedelic approved for treatment resistant depression, and ketamine (generic) is used off-label.
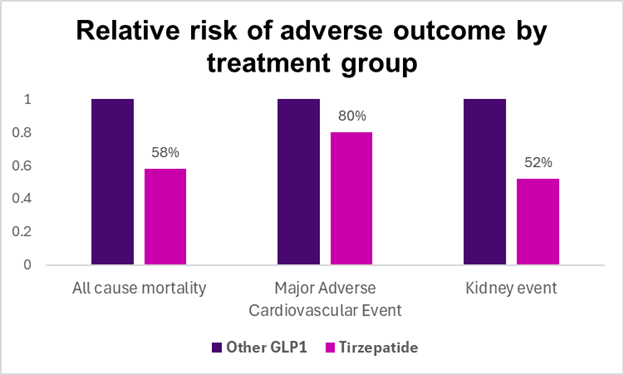
E) Tirzepatide lowers mortality and adverse events in those with diabetes
Researchers reviewed deidentified medical records from about 14,000 people with diabetes treated with tirzepatide and about 14,000 matched people with diabetes who were prescribed a different GLP-1 medication around the same time. Both groups were followed for about a year. Even over this short period of time, the likelihood of death, new heart attack, and new stroke was statistically significantly lower in those who took tirzepatide. The difference persisted even when those on non-maximal doses of the other GLP-1 medications were removed from the analysis. Clinicians are more likely to prescribe tirzepatide for diabetes given this positive observational study, although randomized controlled trials would be more convincing. The research was published in JAMA Network Open.
Source: Chuang, JAMA Network Open August 12, 2024 LINK