

Shorts: Pedi vaccinations, sterilizations,gender affirming care and preventive care requirement
January 24, 2025

A. Pediatric vaccination rates declining
Declining rate of selected pediatric vaccinations
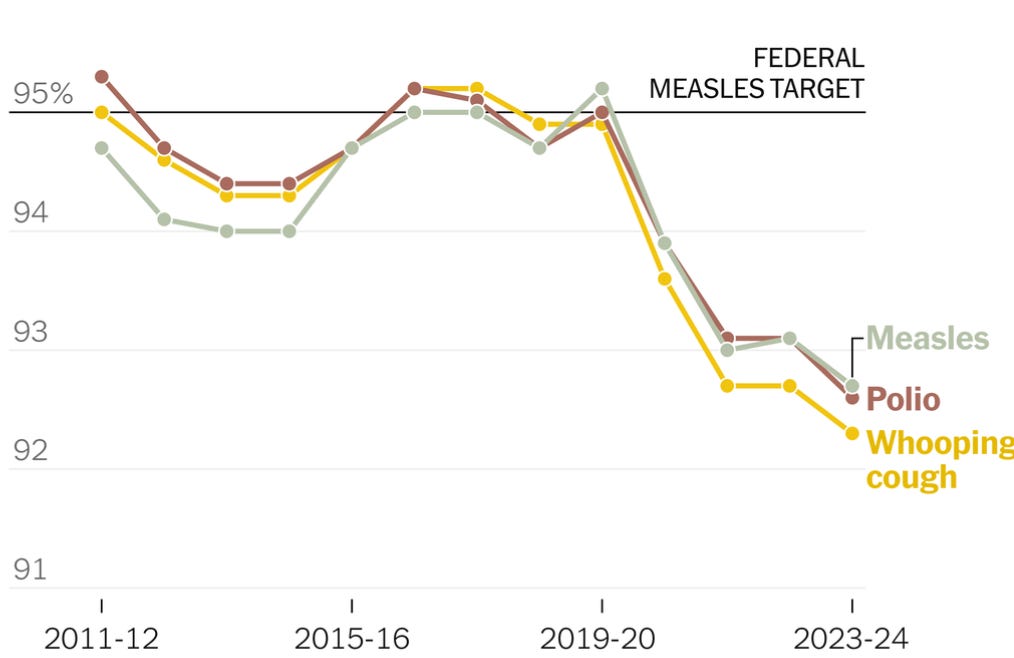
Source: CDC Data via the New York Times, January 13, 2025. Note that the “y” axis does not start at zero. Population vaccination rates of less than 92-95% make measles epidemics likely.
High vaccination rates protect the entire community. When vaccination rates fall, even some of those who were previously vaccinated as their immunity may have waned. Many specific areas and schools already have vaccination rates dangerously below 90%. Epidemics of preventable childhood illnesses could lead to bad outcomes for children and also could lead to more time away from work for parents and decreased economic output.
B. Rate of permanent sterilizations rising among young adults
Visits for sterilizations

Source: Strasser, et al Health Affairs, January 2025
Research published in this month’s Health Affairs shows that the rates of permanent sterilization (tubal ligation in women and vasectomy in men) have increased since the Dobbs decision allowed states to severely restrict or ban abortion. This effect was more pronounced in states the authors judged were more likely to restrict the right to reproductive services. Nonetheless, other studies have demonstrated an increase in birth rates in states with severe abortion restrictions or bans. These changes could impact medical claims experience in employer-sponsored health insurance.
C. Few minors obtain gender affirming medications
Gender affirming care for minors has been in the news, and researchers in JAMA Pediatrics just published a claims data report demonstrating that treatment with hormones for gender dysphoria is rare among those under 18. This was a claims study, so the researchers could not ascertain each person’s diagnosis, so this might slightly overestimate gender affirming treatment.
The researchers reviewed a private insurance claims database with over 5 million adolescents (and almost 12 million person-years of experience.) They found that no child under age 12 received gender affirming hormones, and the rate of those receiving such therapy between ages 14 and 18 were 50/100,000 (0.05%) for children assigned female at birth, and 25/100,000 (0.025%) for children assigned male at birth. Most of the prescriptions were filled for teens over years of age.
Puberty blockers were also only used rarely. Such prescriptions were filled by 21/100,000 (0.021%) of children assigned female at birth, and 15/100,000 (0.015%) of children assigned male at birth. These medications are given at the start of puberty, if they are given at all.
Here’s a link to a previous post about the rarity of any type of gender affirming surgery in those who are under the age of 18.
D. Supreme Court to rule on Affordable Care Act’s preventive care requirement
The Supreme Court announced last week that it will hear arguments on Becerra v. Braidwood Management, a case that challenges the ACA’s requirement that employers waive cost sharing on preventive services that have been recommended by the U.S. Preventive Services Task Force, the Health Services Resources Administration, and the Advisory Committee on Immunization practices. The oral arguments will be this fall, and a ruling is not expected until Spring 2026.
Here’s a link to a previous post on waived cost sharing for HIV prevention drugs.
Preventive care costs employers little, and some elements of preventive care (childhood vaccinations and contraception) lower the cost of care for the population. I’ll have more to say on this in the coming weeks.