Statins effectively reduce cardiovascular risk in people with diabetes, regardless of baseline risk level
February 4, 2026

Summary: A study showed that statins reduce mortality and cardiovascular events in people with diabetes, but the absolute benefit is modest among those at low baseline cardiovascular risk.
Vincent Ka Chun Yan, Joseph Edgar Blais, John-Michael Gamble, et al. Effectiveness and Safety of Statins in Type 2 Diabetes According to Baseline Cardiovascular Risk: A Target Trial Emulation Study. Ann Intern Med. December 30, 2025. Risk expressed as risk of a cardiovascular event in the following ten years.
Those with type 2 diabetes (T2DM) are at higher risk of cardiovascular disease, and treatment with statins can reduce that risk. However, multiple competing guidelines recommend different thresholds for treatment. For instance, the American Heart Association and the American College of Cardiology recommend statin treatment for all people with T2DM between ages 40-75, while the U.S. Preventive Services Task Force recommends treatment only for those with diabetes who are estimated to have a 10% or greater risk of a major cardiovascular event in the next ten years.
Research published in Annals of Internal Medicine used a large U.K. electronic health record database to match adults aged 25–75 with type 2 diabetes mellitus who initiated statin therapy to comparable patients across levels of cardiovascular risk who did not initiate statins. Patients were matched for demographics (age, gender, ethnicity), clinical factors (obesity, hypertension) and social factors (such as whether they lived in disadvantaged communities.)
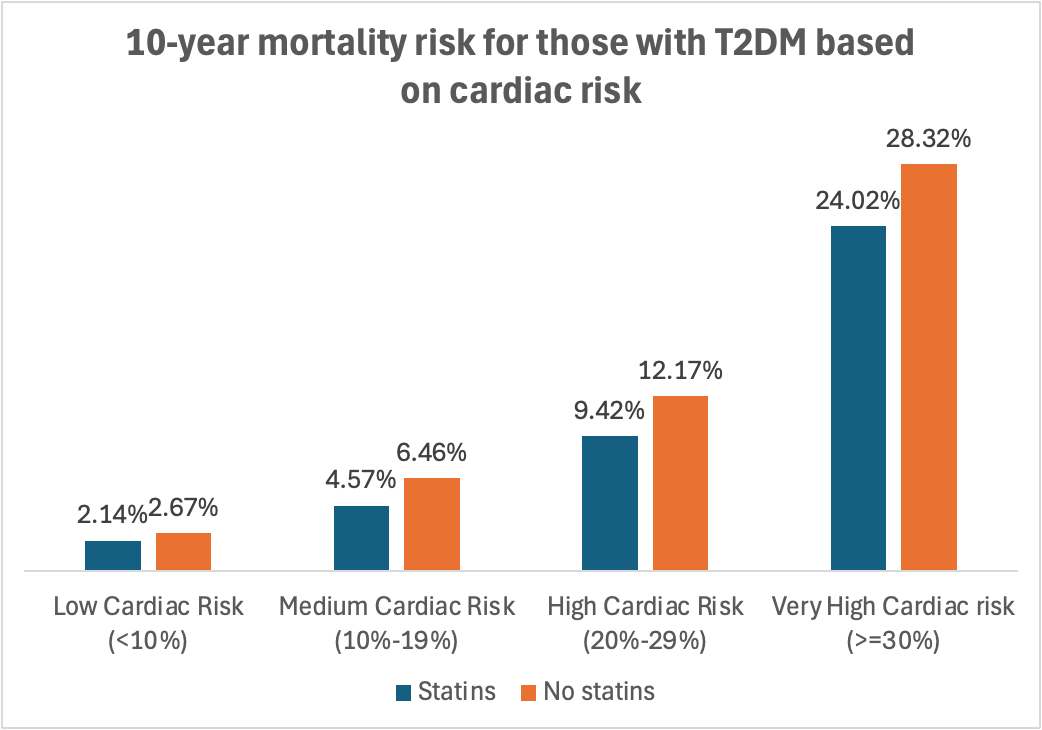
They found that statin use lowered the risk of cardiovascular events and death for those in all risk groups, even those at the lowest baseline risk. Statin therapy was not associated with liver dysfunction in any risk group, and was associated with a small increase in muscle symptoms (myopathy) in the moderate risk group only. The authors conclude that statins are safe, and present this data to help clinicians and patients make decisions about whether to initiate statin therapy.
Another useful metric is the ‘number needed to treat’ (NNT), which I calculated from the results reported in this study.
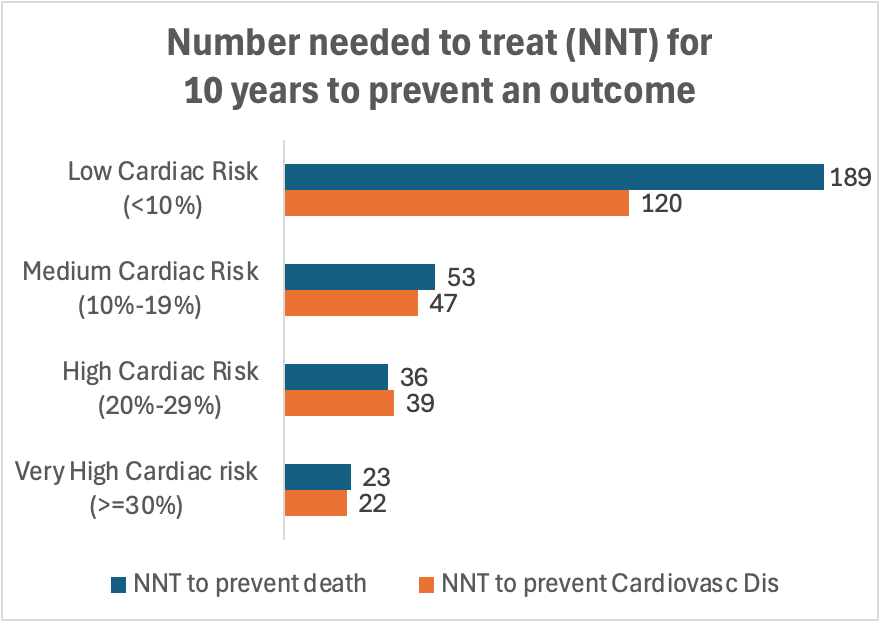
NNT is calculated as one divided by the absolute difference in event rates between treated and untreated patients. For example, among patients at low baseline cardiovascular risk, the 10-year mortality rate was 2.67% without statins versus 2.14% with statins, an absolute risk reduction of 0.53%. This corresponds to an NNT (1/0.53%) of 189 to prevent one death over 10 years.
If the incremental cost of statin treatment is approximately $250 per year—including medication, laboratory testing, and occasional additional office visits—the cost of preventing a cardiovascular event ranges from about $54,000 for those at very high risk to roughly $472,000 for those at low risk. My calculations are here.
Implications for employers:
Statins can prevent both cardiovascular events and death in those with T2DM, even those at low baseline risk.
Employers can ask health plans to report the proportion of members with diabetes who are treated with statins.
The NNT illustrates that many more low-risk individuals must be treated to prevent an adverse outcome compared with treating higher-risk patients.
Individual patients and their clinicians should be aware of how likely treatment is to help an individual, and policymakers should be aware of the high cost of preventive treatment for those who are at low risk of an adverse outcome.