

Study does not show cost savings from digital hypertension interventions
November 1, 2024

Summary: Digital interventions for high blood pressure are associated with higher short-term total cost of care.
Source: Peterson Health Technology Institute, October 28, 2024
High blood pressure is common, affecting 120 million American adults, and increases the risk of heart attacks, strokes, kidney disease, and premature death. Many with hypertension remain undiagnosed, and many are not treated adequately to reduce their risks. The National Committee on Quality Assurance (NCQA) reported that in 2022 only 45% of those with diagnosed hypertension had a blood pressure under 140/90 at their last office visit.
The Peterson Health Technology Institute (PHTI) published its report on digital hypertension interventions earlier this week. This is the third report on digital medical interventions the group has produced this year; previously PHTI reported on digital interventions for diabetes and musculoskeletal disease. This report provided findings on three categories of digital hypertension interventions:
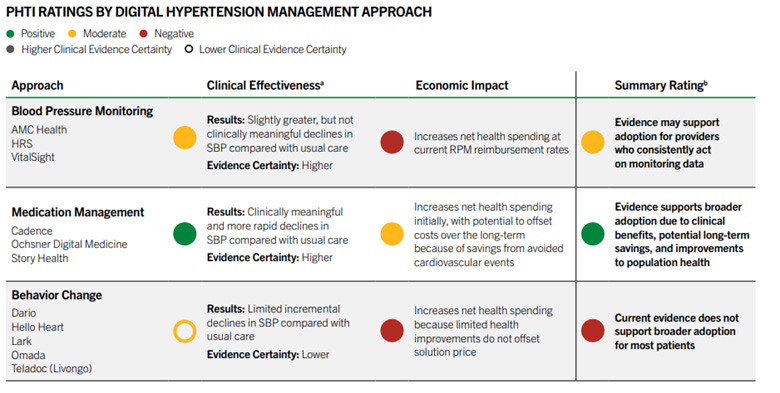
Blood pressure monitoring. Programs to provide home blood pressure monitors, often transmitting readings to a provider. They found that these programs were associated with small decreases in blood pressure, not enough to make a clinical difference across a population in most instances.
Medication management: Offering dedicated provider teams to adjust blood pressure medications was associated with meaningful decreases in blood pressure.
Behavioral change: Patient education and coaching programs and self-monitoring to drive better self-management led to only small changes in blood pressure, again not enough to make a clinical difference across a population in most instances.
The blood pressure monitoring services reviewed in this study are arranged through a provider system. Some of the medication management programs (Story Health and Ochsner) are marketed to employers. All of the behavioral change programs are sold directly to employers. Behavioral change vendors reviewed include Dario, Hello Heart, Lark, Omada, and Teladoc (Livongo).
PHTI performed economic modeling on these three models, assessing financial benefit (such as fewer heart attacks) and costs (vendor costs, when these were available). They did not consider any increase in the cost of antihypertensive medications based on increased adherence, but these costs would be low as most blood pressure medications are inexpensive generics. They reported that all these interventions increased medical costs over the short run (3 years), although there was potential that medication management would lower costs over a longer time period.
The PHTI report includes references to vendor studies projecting lower total medical expenses published by many of the vendors, although notes that many of these studies have a high risk of bias, few fully describe the matched control population, and vendor publications often do not include vendor costs. In some instances, the source of savings (for instance decreased surgical costs) did not match likely outcomes of the interventions.
Implications for employers:
- Medication management programs to optimize provider prescribing showed the most promise at clinical improvement, and carriers can consider reimbursing providers for these programs.
- Employers should review the PHTI findings as they consider hypertension programs. A more intensive program is likely to improve blood pressure and decrease major adverse cardiovascular events, although most programs are unlikely to lower short term medical costs.
- Employers can speak to their carriers about how those carriers are encouraging Value-Based Contracts, which can make it easier for PCPs to develop hypertension programs that may create more value at the routine provider level.
- Few medical interventions are cost-saving; most are at best cost-effective. Well-designed and well-executed digital blood pressure interventions could improve and save lives even if they do not lower medical costs.
- Many digital interventions come with a performance guarantee (PG) for monetary savings. Employers should critically review the methodology of such PGs.
Thanks for reading. You can find previous posts in the Employer Coverage archive
Please subscribe, “like” and suggest this newsletter to friends and colleagues. Thanks!
Monday: IRS expands allowable preventive care without cost-sharing