Time to end COVID-19 vaccine mandates? Also brief notes on polio and brain fog.
September 16, 2022

Happy Friday!
Today, I’ll go over some thoughts on vaccine mandates as we head into our third autumn of the pandemic, review what the outbreak of polio in New York means for employers, and offer some follow up on Long COVID.
1. Vaccine mandates did their job, but are no longer necessary for many employers
There were strong reasons for many employers to implement vaccine mandates in the fall of 2021. COVID-19 was an exceptionally deadly disease, available treatments weren’t very good, unvaccinated workers were more likely to bring the virus into the workplace, and immunity rates in the population were low. A government requirement for mandates appeared likely for many employers.
Today, the world is a different place. COVID-19 remains more deadly than influenza, but those dying are largely elderly or have compromised immune systems. In Massachusetts over the last two weeks, for instance, 91% of deaths have been in those aged over 70, who represent just 11.6% of the population. The monoclonal antibody Evusheld provides some degree of protection for those with immune compromise, and drugs like Paxlovid dramatically decrease risk of hospitalization or death. Those who are unvaccinated remain more likely to get COVID-19 and be infectious, but the difference in infection rate between vaccinated and unvaccinated people is now much smaller. Immunity rates, from vaccination, infection, or both, are high.
Prior employer vaccine mandates have substantially increased employee vaccination rates. Based on a study of college vaccine mandates, employer vaccine mandates likely saved at least tens of thousands of lives. Employees at workplaces with mandates generally supported these, and many were vaccinated earlier than they would have been. Of note, government mandates remain in effect for many government employees and health care workers.
But employers have used substantial administrative resources to implement and maintain these mandates and have generally not expanded the mandate to include boosters. About 30% of adults 18-64 received even a single booster, and it will be a challenge to get a majority of adults to get the new bivalent booster which provides protection against Omicron strains BA.4 and BA.5. (I got my bivalent booster on Monday, had no adverse effects beyond a sore arm, and strongly recommend that those more than 2 months from their last COVID-19 shots or infection get this booster).
At this point, a mandate to have the initial vaccination without boosters doesn’t make clinical sense, since those who were vaccinated many months or even over a year ago have little remaining immunity from that vaccination. But employers are unlikely to voluntarily implement a mandate to obtain the new booster shot at this point, with the danger from COVID-19 substantially lower than it was a year ago.
Some employers should maintain COVID-19 vaccine mandates, including hospitals and nursing homes (required to by the Centers for Medicare and Medicaid Services, CMS). The hospitals where I am on staff require that employees and staff are up to date with boosters as well as initial vaccination. Congregate living workplaces (including senior care and prisons) would be safer for all if they had mandates in place, although many have already removed these.
COVID-19 is still a serious health threat, and community transmission remains high in over 80% of counties. And there is plenty that employers can do to keep the workplace safe! Employers can:
- Promote influenza vaccine. (Co-infection with COVID-19 and influenza is especially deadly). Some employers have returned to flu shot clinics this fall, with more workers back at the workplace.
- Promote the COVID-19 bivalent booster, which is widely available in pharmacies and medical facilities. Fewer employers will do COVID-19 vaccine clinics, though, as refrigeration requirements are more demanding and this vaccine requires 15 minutes of observation, which complicates vaccine clinic logistics.
- Be mask-friendly and consider mask requirements if there is a large community outbreak or for large indoor gatherings.
- Offer sick leave to encourage those with respiratory illnesses not to come to the workplace
- Increase ventilation, and carefully monitor indoor air quality.
- Maintain flexibility to allow remote work where possible. This reduces employee density and further encourages employees not to come to the workplace if ill or if they recently had a high-level exposure.
- Encourage employees to do over-the-counter COVID-19 tests if they feel ill, five days after known exposure, and before and after business travel. Remind employees that employer sponsored health plans offer 8 over-the-counter tests monthly for each insured member. We have reviewed claims data showing that less than 1% of members have obtained these tests each month since this requirement began early this year.
Here’s data from Canada published in early September, showing that those with 4 doses of vaccine were about 10 times less likely to die of COVID-19 than those with fewer than 2 doses of vaccine at all ages. Canadians who were unvaccinated were also about three times more likely to get a symptomatic infection when exposed. Those in the US overall were 2.8 times more likely to die of COVID-19 than those in Canada.
This shows, for instance, that for those ages 40-49 who were infected with COVID-19, one in 614 unvaccinated died of COVID-19, while one in 5581 who had 4 doses of vaccine and got an infection died of COVID-19.
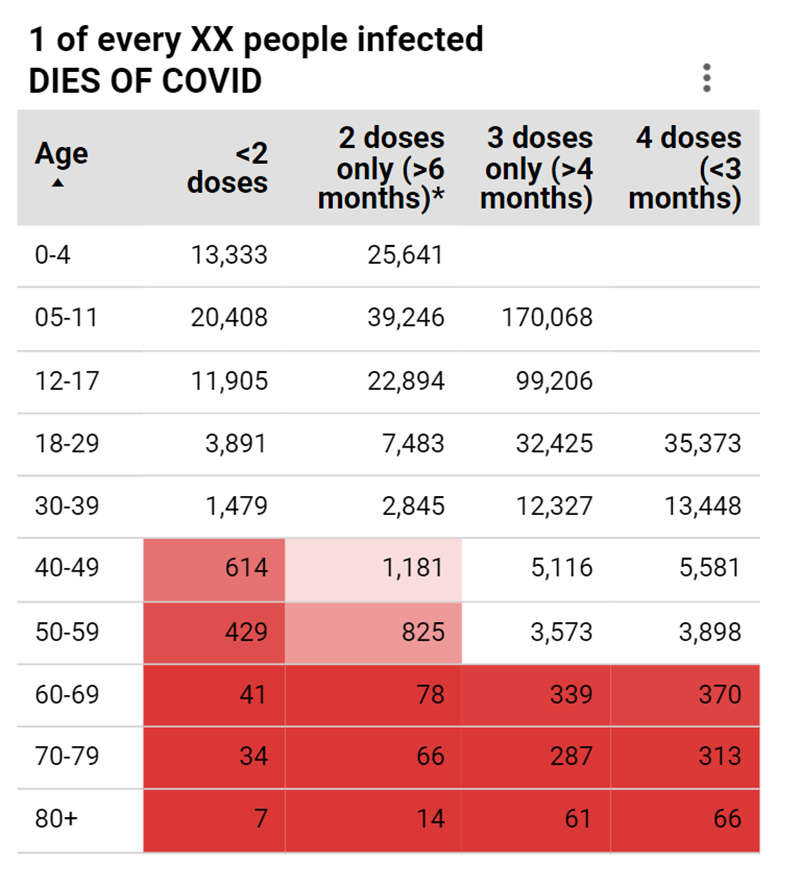
Source: COVID-19 Resources Canada, September 9, 2022 LINK to data LINK to overall document
2. Polio declared a public health emergency in New York
There has not been a second case of paralytic polio following the initial case reported in June, but polio virus has been found in wastewater in New York City and four suburban counties. New York State declared polio a public health emergency on September 9. High vaccination rates in most communities will probably prevent large outbreaks of polio in the US, but those who are unvaccinated remain at risk.
The inactivated polio vaccine available in the United States, which is an injection, cannot cause polio. You might have read that the paralytic polio case was infected with “vaccine derived polio.” This is because a live, oral vaccination used in developing countries can rarely mutate and cause infection. The New York patient probably caught the infection from someone who had a very rare infection from an oral vaccine given elsewhere. No one should worry that their children will catch polio from the vaccine available here. Rather the polio vaccine available in the US and Europe protects very effectively against all strains of the polio virus
Polio vaccines are covered without out-of-pocket costs by employer sponsored health insurance and are mainly administered to children. They are required for school attendance in many states.
Employers should continue to encourage all recommended vaccinations and should require their health plans to report on vaccination rates as part of quality reporting.
Resources for employers:
- Center for Disease Control and Prevention: About Polio
- Advisory Committee on Immunization Practices: Polio Vaccine Recommendations
- European CDC Polio Fact Sheet
- Kaiser Health News Frequently Asked Questions
3. “Brain fog” is really a disorder of executive function
Estimates of Long COVID vary widely, largely because definitions are not consistent, and some of the symptoms were prevalent in the general population before the pandemic. Those with Long COVID often have trouble obtaining work accommodations and disability payments because there is no definitive test.
Ed Yong of The Atlantic describes the challenges and disabilities of those with “brain fog.” He said this of one of his interviewees:
She once worked in artificial intelligence and analyzed complex systems without hesitation, but now “runs into a mental wall” when faced with tasks as simple as filling out forms. Her memory, once vivid, feels frayed and fleeting. Former mundanities—buying food, making meals, cleaning up—can be agonizingly difficult…The fog “is so encompassing,” she told me, “it affects every area of my life.”
Employers can expect an increased rate of requests for work accommodations over the coming months and years. They may want to modify their policies and procedures based on the emerging understanding of Long COVID.
4. Vaccination provides protection against Long COVID
Research from the United Kingdom shows that those who are unvaccinated appear to be about 50% more likely to get Long COVID than those who are vaccinated. Researchers compared extensive follow-up of about 3100 COVID infections in people who were vaccinated with matched unvaccinated patients from a large database of randomly recruited UK residents conducted by the Office of National Statistics.
Employer efforts to increase vaccination rates can help prevent Long COVID, too.
Have a great weekend
Jeff