

Indoor clean air, workplace discrimination and hypertension, over the counter birth control, racial disparities in substance use treatment, and preventive care rules
May 19, 2023

Happy Friday!
Today, I’ll discuss the new Centers for Disease Control and Prevention (CDC) guidelines for clean indoor air, research that shows incidence of subsequent high blood pressure is significantly higher in those who reported discrimination at work eight years earlier, and what OTC birth control means for employers. I’ll also discuss new research about disparities in treatment for opioid use disorder, and the latest in the tangled web of litigation against the Affordable Care Act’s requirement to cover certain preventive services.
1. CDC issues new guidelines for clean indoor air in the workplace
The CDC issued new guidelines for air exchanges and air filtration this week which could help decrease the spread of COVID-19 and other respiratory diseases. The American Society of Heat, Refrigeration and Air Conditioning Engineers (ASHRAE) also issued new draft standards that would require higher levels of air exchanges in schools, hospitals and workplaces.
The CDC guidelines are just that - they are not enforceable regulations. Still, building operators now have clear guidance to aim for five complete air exchanges per hour, which is consistent with what public health experts recommend. The ASHRA draft standards will likely be finalized by summer, and are often the basis of building codes.
This is excellent news. More air exchanges can prevent transmission of COVID-19, influenza, RSV and other respiratory viruses. Better filtration will also limit exposure to p2.5 particles from air pollution; these increase the risk of heart and lung disease. Better quality indoor air has also been associated with better ability to concentrate which can improve productivity.
There is a cost to improving the quality of indoor air. Bringing in more outdoor air means conditioning it (heating in the winter and cooling in the summer), and higher efficiency filters make air handling units work harder. Nonetheless, many companies can make small adjustments to their existing air handling systems to improve indoor air quality.
I’ve been carrying around a carbon dioxide meter to assess whether there are enough air exchanges in small conference rooms. We all exhale carbon dioxide, so this is a good proxy for whether there are enough air exchanges. Last week, I was in a business meeting with about 8 others and the initial CO2 level was 600 (outdoor is 400 - and up to 800 is fine, while over 1000 means there is not enough air exchange.) Midway through the meeting I saw the meter edging up past 1100, and we were able to open the door. The CO2 level went down to under 700 within two minutes. Sometimes it takes very little to improve indoor air quality.
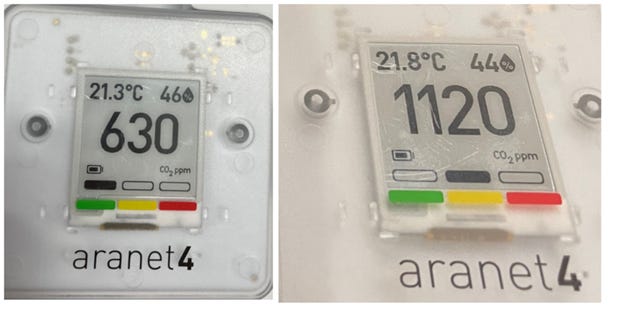
Photos of the carbon dioxide meter that I bring to in-person meetings. Note that carbon dioxide at levels of over 1000 is not harmful, but is an indication that the air is not being exchanged effectively so the risk of transmitting a viral illness is higher. Simply opening a door can often help!
Some schools have installed CO2 monitors in classrooms to demonstrate their concern for clean indoor air. Here’s a link to the public-facing website where the Boston Public Schools disclose indoor air quality.
Implications for employers:
- Following current CDC guidelines, even in buildings where this is not a legal requirement, can reduce worker illness and improve productivity and happiness
- Companies can install CO2 monitors in portions of the workplace that are high risk, such as small break rooms or crowded factory floors.
- Companies can communicate about their efforts to offer cleaner air to demonstrate their concern for employee wellbeing.
2. Workplace discrimination associated with an elevated risk of future hypertension
Researchers reported in the Journal of the American Heart Association that employees who faced a high or moderate amount of discrimination in the workplace were more likely to have hypertension eight years later. The study followed over 1200 employees and used a standardized questionnaire about discrimination, although the reporting of discrimination was higher than anticipated. The researchers excluded those with pre-existing hypertension, and using a smaller sample and more extensive risk adjustment made the findings even more significant. The researchers did not distinguish among discrimination based on age, race, gender, sexual preference, or any other characteristic. This study suggests, but does not prove, that discrimination causes hypertension.

Incidence of hypertension per 1000 person years. Source: Li, et al, JAHA April 26, 2023 LINK
This means that about 39% of those who were subject to a high level of workplace discrimination would have hypertension 10 years later.
Implications for employers:
- Employers that foster an inclusive environment can decrease stress and improve productivity and retention. This study also suggests that there might be a health benefit to eliminating discrimination in the workplace.
- The authors point out that cognitive behavioral stress management training can help make individual employees better able to cope with stress including discrimination at work, but this is no substitute for addressing discrimination.
My WTW colleague Alaina Melena, who leads the Diversity, Equity and Inclusion practice, offers these tips for preventing discrimination and fostering a respectful workplace:
- Be aware of local, state, and federal laws regarding non-discrimination in the workplace
- Develop and enforce anti-discrimination policies. Policies should include a commitment to zero-tolerance for discrimination, outline prohibited behaviors and include all protected characteristics such as race, gender, age, sexual orientation, disability and religion
- Communicate the policy and provide regular training on harassment and discrimination prevention and inclusivity
- Establish a safe and confidential mechanism for employees to raise concerns or complaints regarding discrimination – and act promptly on reports of discrimination
- Regularly assess workplace policies, environment, and employee feedback
3. Food and Drug Administration (FDA) poised to approve over the counter oral contraceptives
An FDA advisory committee unanimously recommended that Opill, a progesterone-only birth control pill, be made available over the counter. Oral contraception has been available without prescription for decades in Europe, and OTC availability of Opill was supported by professional societies including the American Medical Association and the American College of Obstetrics and Gynecology. Most countries do not require prescriptions for contraceptive pills.
The FDA will still likely not make its final decision for months, so it could be late this year before these pills are available. Another company is likely to seek approval for a combination estrogen-progesterone pill in the coming months. The combination pill has less breakthrough bleeding, although it is associated with a higher risk of blood clots, especially in those who smoke.
Over the counter access to birth control is especially important since the closure of women’s health clinics due to abortion restrictions in many states has led to less access for all types of reproductive health.
Implications for employers:
- The FDA has not yet issued a final approval of over-the-counter birth control pills, but this is expected towards the end of 2023.
- Employer-sponsored health insurance covers prescribed birth control pills without any cost sharing, but employers should check with their pharmacy benefit managers to see if their plans will cover over the counter contraception. Most plans do not provide coverage for over-the-counter drugs, such as anti-inflammatory drugs (like ibuprofen) and anti-ulcer drugs (like omeprazole.)
4. Underuse and racial disparities persist in treatment for opioid use disorder
The New England Journal of Medicine published research on individuals on Medicare with disabilities (average age 51) to assess how frequently these patients were treated with buprenorphine (Suboxone) after they had an index event like an overdose, a rehab stay, or an infection due to IV drug use. Buprenorphine is the foundation of Medication Assisted Therapy (MAT), which has been demonstrated to decrease overdoses and save lives in those who have opioid use disorder (OUD).
The results aren’t pretty! Overall, less than one in five (18.2%) received buprenorphine within 180 days of the index event, and there were stark disparities.
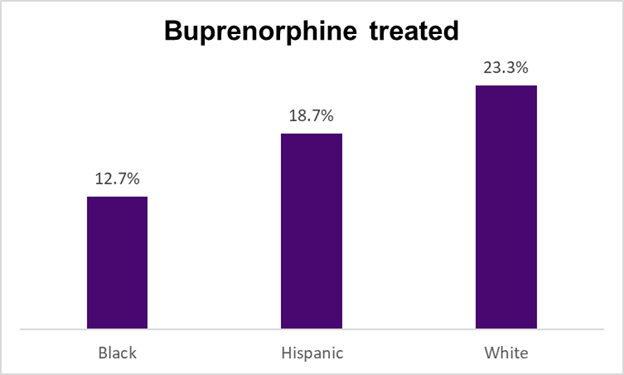
Source: Barnett, et al NEJM May 11, 2023 LINK
On the (a little) brighter side, the rates of buprenorphine use went up between 2016-2019, the years of this study. Further, the increase was greater in Black people than in White people, so the disparities are (a little) less.
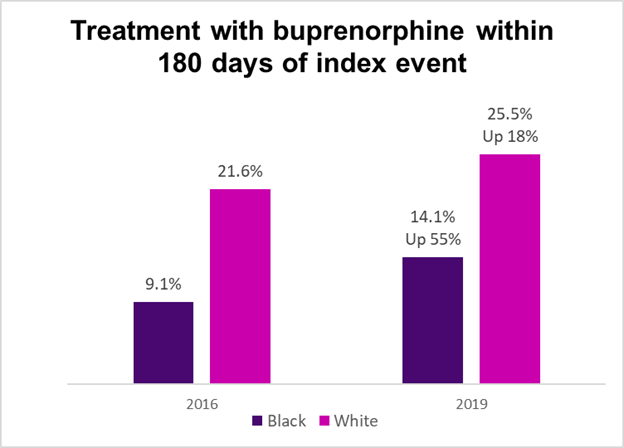
Source: Barnett, et al NEJM May 11, 2023 LINK
Drug overdose deaths exceeded 100,000 last year, and this is a major issue for employers as drug overdoses wreak havoc on the family and on the workplace. Barriers to treatment of OUD have diminished in recent years. Elimination of the training requirement for physicians will hopefully increase the number of prescribers for these life-saving medications, and at least for now telemedicine to prescribe buprenorphine has been extended.
Implications for employers:
- Some employers encourage the use of MAT by offering these prescriptions without cost-sharing. This could also diminish disparities.
- Naloxone (which can be used to treat acute opioid overdoses) has also been FDA approved for over-the-counter use and will be available in late summer. Making naloxone part of workplace first aid kits can save lives. When people have been treated for a drug overdose with naloxone, they should usually be treated subsequently with MAT.
- Substance use treatment is often hard to find, and there are many out-of-plan providers who offer programs that are expensive and not evidence-based. Employers can check with their carriers to be sure that there is adequate access to substance use treatment.
- Employers can also ask carriers or pharmacy benefit managers to report on the number of members who are receiving MAT, and adherence to therapy.
5. No change in requirements to provide certain preventive services with no out of pocket costs (for now)
The Fifth Circuit Court of Appeals granted the Biden Administration a stay on the District Court ruling (Braidwood Management vs. Becerra) that would have discontinued the Affordable Care Act’s requirement of coverage without cost sharing for a number of preventive services. Therefore, coverage of all ACA required preventive care remains mandated (except for the company that challenged the requirement.)
As I’ve noted before, the total cost to employers of covering this preventive care is low, and these preventive services are frequently used and are valued by employees. In many instances, they can prevent illness and even save lives. The Fifth Circuit has paused the ruling until it can hear and decide the appeal, and the case is likely to be escalated to the Supreme Court, so it’s likely there will not be a final determination in this case until long after 2024 benefits are set.
Have a great weekend when it comes!
Jeff